Placental, Morphological, and Ultrasonographical
Particularities in Post-Term Pregnancies
Carmen Mihaela MIHU, Dan MIHU
“Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
Abstract
Post-term pregnancies are evaluated, using 2D and Doppler ultrasonography. Apparition of fetal distress is certified by the increase of PRI. The current study aimed to establish a relationship between the ultrasonographical particularities of placentae and morphologic and morphometric aspects noticed in placentae postpartum.
Keywords
Ultrasonograhy; Placenta; Mophometric Measurement
Introduction
Normal pregnancy lasts about 40 weeks of amenorheea (WA). The risc of fetal complications increases during the pregnancies, which exceed this period.
After the median term of 40 WA, pregnant women can be examined using 2D and Doppler ultrasonography, determining the placental resistivity index (PRI). After 40 WA, PRI does not decrease; its tendency is to be increased after 42 WA.
Fetal distress (FD) cannot be installed if the values of PRI are lower than 0.64. In this way, we can estimate the debut of fetal distress, by repeating each day the Doppler examination.
Material and Methods
There were 10 cases of pregnancies, which exceeded 40 WA, included in this study.
All were normal pregnancies. The gestational age was determined correlating anamnestic datas (first day of last menstruation) with echographic biometry datas, evaluated before 20 WA (cranio-pelvic length, biparietal diameter, femural length).
2D ultrasonography was performed by a Ultramark 9 with transductor of 3.5 MHz, with color and pulsatile Doppler, coupled with a real time B ultrasonograph; and a Medisson Sonoace 8800 with transductor of 3,5 MHz, with color and pulsatile Doppler; coupled with a real time B ultrasonograph.
Morphologic and morphometric analysis was performed on placentae. Placentae were fixed in neutral 10% formaldehyde. They were macroscopically analysed and their weight, thickness at the point of umbilical cordon insertion, and placental diameter were measured. Fragments from different parts of placenta were collected, included in wax, realizing three blocks for each placenta. They were colored in HE, PAS, red Sirius and orchid colorations. 3-4 lamas were selected of each block, which were microscopically examined at a BX50 Olimpus microscope. Hystopathological particularities were observed and morphometric measurements were performed.
Results
2D ultrasonography particularities
Placental maturation. 2D ultrasonographic evaluation, according to Kazzi classification, suggested the following particularities of placentae’s structure:
· 3 intermediary placentae;
· 7 mature placentae (Fig. 1, 2, 3).

Fig. 1. Pregnancy 41 WA

Fig. 2. Pregnancy 41 WA+ 4 days
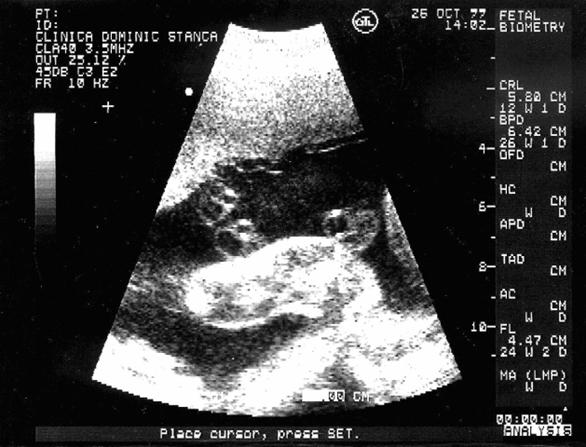
Fig. 3. Pregnancy 41 WA + 5 days
Placental thickness, ultrasonographically measured, were presented in Table 1.
|
Case |
Placental thickness at different gestational ages (mm) |
|||
|
40 WA to 40 WA + 5 days |
40 WA + 6 days to 41 WA + 1 day |
41 WA + 2 days to 41 WA + 4 days |
41 WA + 5 days to 42 WA + 3 days |
|
|
1 |
38 |
38 |
37 |
37 |
|
2 |
36 |
35 |
35 |
35 |
|
3 |
38 |
37 |
37 |
37 |
|
4 |
35 |
35 |
35 |
35 |
|
5 |
37 |
35 |
35 |
35 |
|
6 |
40 |
38 |
37 |
37 |
|
7 |
34 |
34 |
34 |
34 |
|
8 |
36 |
35 |
34 |
34 |
|
9 |
35 |
34 |
34 |
34 |
|
10 |
35 |
34 |
34 |
34 |
Table 1. Placental thickness at different gestational ages
Doppler ultrasonography particularities
For each case, median values of PRI were calculated.
Out of 10 cases of pregnancies, which exceeded 40 WA, 6 were interpreted as real post-terms (Fig 4, 5). Four pregnancies were considered as chronological post-terms. Threshold value of PRI was 0.64.
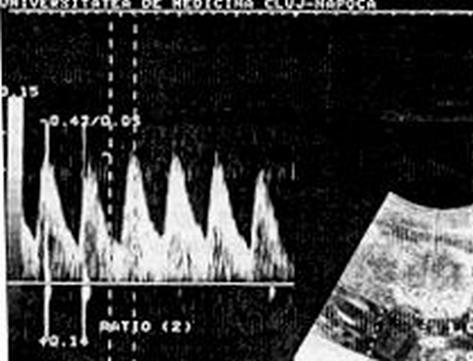
Fig. 4. Doppler ultrasonography – umbilical artery
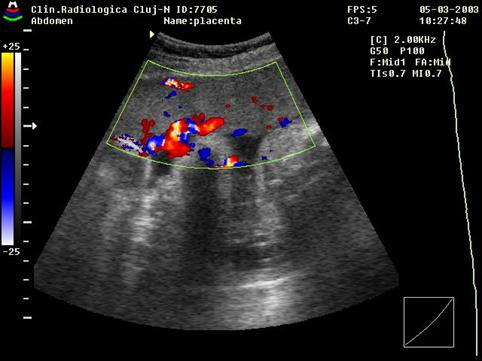
Fig 5. Color Doppler ultrasonography - Intraplacental circulation
Three situations were recorded in these conditions:
· PRI value is 0.64 and tends to decrease.
· PRI value is 0.64 and remains constant.
· PRI value is 0.64 and it remains constant or even increases.
The values of PRI were presented in table 2.
|
Number of cases |
Minimal value of PRI |
Maximal value of PRI |
Average value of PRI |
|
2 |
0.59 |
0.68 |
0.63 |
|
4 |
0.56 |
0.65 |
0.60 |
|
3 |
0.58 |
0.64 |
0.61 |
|
1 |
0.60 |
0.67 |
0.63 |
Table 2. The minimum, the maximum and the average values of PRI
in different gestational ages.
Placental morphologic aspects
Macroscopical examination of placentae offered the data presented in table 3.
|
Case |
Average Weight of Placenta (g) |
Average Thickness of Placenta (mm) |
Average Diameter of Placenta (mm) |
|
1 |
600 |
38 |
180 / 170 |
|
2 |
580 |
35 |
180 / 160 |
|
3 |
580 |
36 |
170 / 170 |
|
4 |
540 |
35 |
160 / 150 |
|
5 |
590 |
36 |
170 / 160 |
|
6 |
600 |
37 |
180 / 180 |
|
7 |
530 |
35 |
160 / 150 |
|
8 |
570 |
34 |
170 / 160 |
|
9 |
550 |
34 |
160 / 160 |
|
10 |
560 |
36 |
150 / 160 |
Table 3. Average weight, thickness, and diameter of placentae.
A slight decrease of placental dimensions was observed, with an average weight of 570 g.
Microscopic examination offered the following aspects:
· progressive degeneration of chorionic villi (Fig. 6);
· diffuse calcifications; (Fig. 7)
· edema;
· intervilli thrombosis;
· infarcts;
· perivilositar deposits of fibrins (Fig. 8).
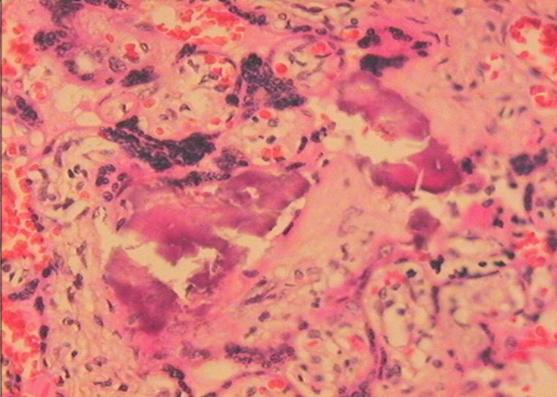
Fig. 6. Vilous degeneration-col. red Sirius
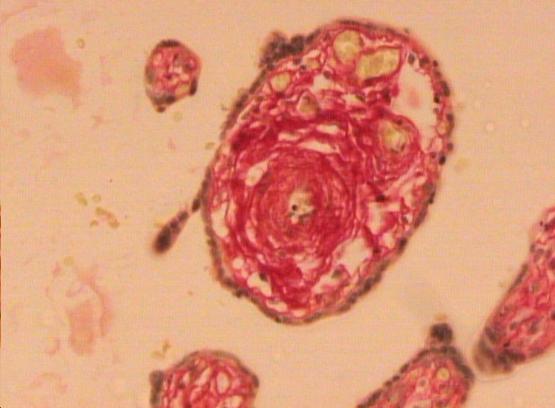
Fig. 7. Diffuse calcifications-col. HE
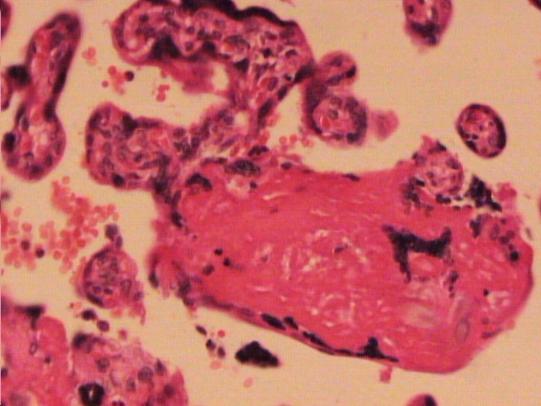
Fig. 8. Deposits of fibrine-col. HE
Morphometric determinations offered the following values (Table 4):
|
Case |
Vessel’s Diameter (μm) |
Wall thickness (μm) |
Luminal Surface (μm2) |
|
1 |
39.05 |
11.12 |
284.33 |
|
2 |
38.65 |
10.97 |
288.04 |
|
3 |
39.64 |
10.25 |
293.33 |
|
4 |
36.55 |
13.10 |
199.62 |
|
5 |
33.49 |
14.65 |
112.45 |
|
6 |
37.12 |
13.68 |
234.61 |
|
7 |
40. 23 |
12.78 |
299.87 |
|
8 |
39.34 |
11.67 |
301.77 |
|
9 |
41.30 |
12.08 |
321. 88 |
|
10 |
40.09 |
14.89 |
288.79 |
Table 4. Results of morphometric measurements
In real cases of post-term, morphometric determinations marked out smaller vascular diameters, bigger vascular wall thickness, compared to normal pregnancies, which implies the decrease perfusion’s surface.
Discussions
Studies of current references describe phenomenae of placental hypermaturation, as a main characteristic of post-term pregnancies [1].
Results obtained after Doppler sonography examination confirm theoretical data which shows an average value of RI of 0.62 after 40 WA [2, 3].
Our study proposes a simple method to examine post-term pregnancies, which is reproducible and non-invasive. Umbilical velocimetry allows analysis of conditions in which feto-placental exchanges are performed, and the moment when placental failure occurs. Ultrasonographic aspects can be correlated with histopathological modifications observed in these placentae.
Some authors propose the value of PRI < 0.64 as a security threshold, eliminating in this way the risk of FD, but Doppler examination must be repeated at an interval of 2 days. If the value of PRI is 0.64, then increase the risk that FD to appear, this risk depends on the evolution of PRI values; the increase of PRI increases the risk of FD [4].
According to these aspects, Doppler examination from the beginning of post-term period makes possible to define fetuses with high PRI, which imposes a careful examination of pregnancies [5, 6].
Current references mention the following in post-term pregnancies:
· Variable intensity colagenisation of chorionic villi stroma, up to hypo or non-cellular total sclerosis;
· Blood vessels present obliterant endotelitis, trombosis with hemosiderin deposits;
· Extended calcification, fibrinoid deposits and beaches of X cells, may appear at vilositar level;
· It is very important to mention that these extended modifications, are associated with “young” vilosities, with rich stroma, limited by normal sincitio-capillarry membranes [7].
In addition, these authors do not point out a clear correlation between the modifications in umbilical velocimetry and anathomopathological aspects of placenta in a post-term pregnancy: thrombosis, alterations of microcirculation [8]. Although, we can affirm that anatomopathological aspects of these placentae are typical for the process of placental senescence.
Conclusions
1. Umbilical velocimetry, can predict the moment when FD occurs.
2. Performing the umbilical Doppler examination at the beginning of post-term, allows defining high PRI pregnancies.
3. When the value of PRI is 0.64, the risk for FD to occur is higher, knowing that PRI tends to increase in the next interval.
4. All anatomopathological aspects, which were observed, are typical for the process of placental senescence.
5. These lesions are more common when velocimetry indexes are altered, confirming placental failure as the cause of CFD in post-term pregnancy.
References
1. Uzan M., Cynober E., Benard C., Guide practique de Doppler en obstétrique, 1992.
2. Pattison R.C., Norman K., Odendaal H.J., The roll of Doppler velocimetry in the management of high risk pregnancies. A randomized controlled trial, J. Matern. Fetal Investing, 1993, 3, p. 182.
3. De Rochambeau B., Jabbour N., Mellier G., La vélocimétrie Dppler ombilical dans la grossesses prolonges, Re. Fr. Gynecol-Obstét, 1992, 5, p. 289-294.
4. Zimmermann P., Alback T., Kovkimen J., Vaalamo P., Tuimala R., Ranta T., Doppler flow velocimetry of the umbilical artery, uteroplacental arteries and fetal middle cerebral artery in prolonged pregnancy, Ultrasound Obstet. Gynecol., 1995, 5, p. 189-197.
5. Devine P.A., Bracero L.A., Lysikiewicz A., Evans R., Middle cerebral to umbilical artery Doppler ratio in post date pregnancies, Obstet. Gynecol., 1994, 84, p. 856-860.
6. Mihu D., Mihu C., Ombilical Doppler Ultrasound Examination in Prolonged Pregnancies, Romania Journal of Ultrasonography, 1999, 1, p. 49-54 (In Romanian).
7. Teodorescu M., Georgescu L., Tudose N., The pathology of Placenta, Facla Publishing House, 1977 (In Romanian).
8. Nimrod C., Gruslin-Giroux A., Post term Pregnancy Chapter In: Copel J.A., Reed K.L. Doppler Ultrasound in Obstetrics and Gynecology, New-York, Raven Press, 1995, 17, p. 165-171.